The Science of Qi: Myofascial Lines and TCM Meridians Compared
TLDR: Research shows an 89% overlap between the 12 acupuncture principal meridians and the nine myofascial meridians identified through anatomical dissection. Acupuncture points cluster at fascial layer intersections, and meridians appear to follow intermuscular connective tissue planes — suggesting that classical Chinese maps of the sinew channels and modern myofascial anatomy are two independent descriptions of the same structural network. Practitioners who understand both systems have a broader clinical map for treating pain that doesn't resolve with local treatment alone.
Part of my doctoral thesis was built around a question that had been quietly nagging at me since my first year of school: what would Chinese medicine look like if it were invented today?
The question sounds provocative, but the intent behind it wasn't. It was an attempt to figure out whether the principles underlying TCM had real structural correlates in modern science, or whether they were purely philosophical constructs that worked clinically for reasons we didn't fully understand. I spent a lot of that time wrestling with qi.
I was frustrated by it. Every instructor I had, when pressed on what qi actually was, would tell me it was energy. And I'd sit there thinking: okay, but what does that mean? Energy is a word that covers an enormous amount of territory in physics. It doesn't tell you anything on its own. I kept pushing, and the answers kept being the same.
Eventually I came around to understanding that they were right, just in a way that wasn't particularly satisfying to a student who wanted precision. Qi, as a concept in ancient China, was used to describe anything that was functionally real but couldn't be named with more specificity. If you didn't have the vocabulary or the instruments to call something "electrical potential" or "chemical gradient" or "kinetic force," you called it qi. The term had to carry all of it. In that sense, qi isn't wrong. It's just one word doing the work that modern science now distributes across a dozen fields. Chemical energy, mechanical energy, electrical signaling, potential energy stored in tensioned tissue — all of it would have been qi to a classical practitioner. We just have better tools now for naming the parts.
That reframe helped me. But where things got genuinely interesting, and where I still find myself thinking about it years into practice, is the meridians. Specifically, the sinew channels.
If you work with both TCM and manual therapy, or if you've spent any time with Thomas Myers' Anatomy Trains, you may have had a moment in the clinic where you noticed the overlap and quietly thought: that's not a coincidence. You were right. It isn't. And the research is starting to say so out loud. The Acupressure and Meridian Massage course covers the clinical logic behind meridian selection in a way that holds up to this kind of scrutiny, if you want to work with it directly.
What the Sinew Channels Actually Are
The sinew channels are a distinct layer of the TCM channel system that maps musculoskeletal anatomy more closely than the primary meridians, making them the most clinically accessible part of Chinese medicine for practitioners treating movement and pain. Most practitioners who study TCM spend the bulk of their channel work on the 12 primary meridians. The sinew channels, or jing jin, tend to get less attention in training. That's a loss.
The sinew channels are described in the Huangdi Neijing Lingshu as a three-dimensional network of muscles, tendons, and connective tissue that follows the pathways of the primary channels but runs more superficially. They don't connect to the internal organs the way the primary channels do. Their work is somatic: movement, posture, joint stability, and pain. A 2022 paper in the Journal of Acupuncture and Meridian Studies noted that sinew channels are better compared to the myofascial system than to the primary acupuncture channels, given the closer functional similarity [6].
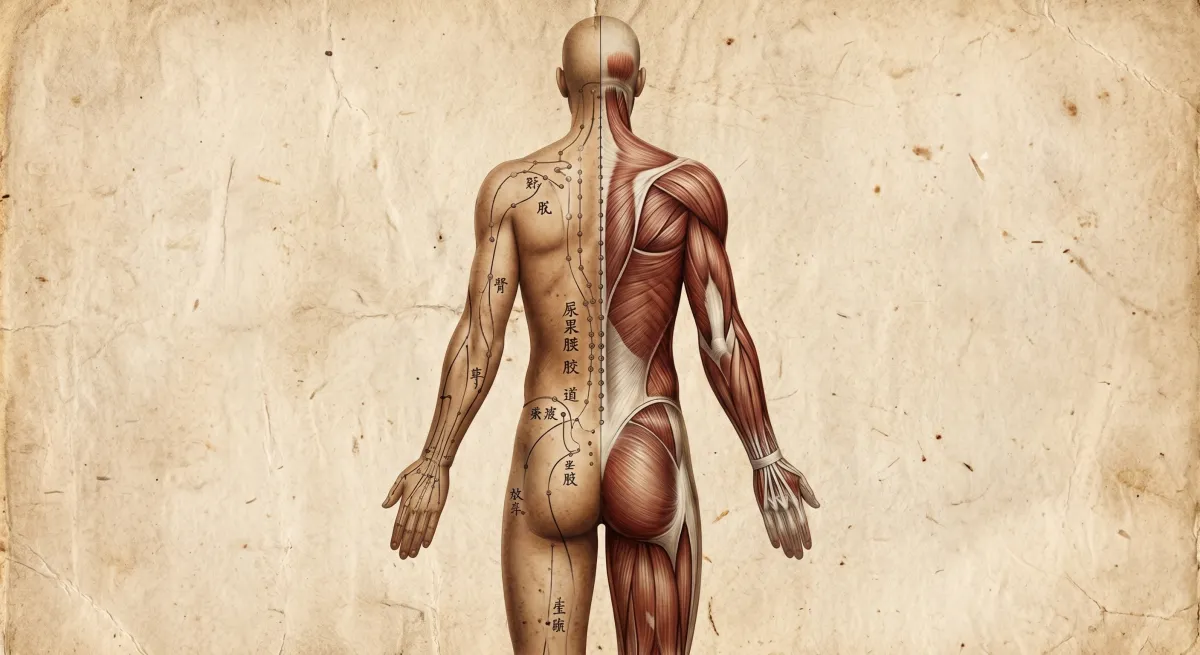
When you read the classical descriptions in the Lingshu, you're reading something that sounds a lot like a fascial anatomy text — a continuous network of tensioned tissue that transmits force, generates postural holding patterns, and refers symptoms across distances that don't follow simple segmental logic.

The sinew channel system as described in the Huangdi Neijing Lingshu. Note the continuous pathways from extremity to trunk.
Where Tom Myers Comes In
Eight of the nine myofascial meridians identified through anatomical dissection show substantial overlap with the 12 acupuncture principal meridians — 89% correspondence across the two systems [5]. A 2009 study in the Journal of Alternative and Complementary Medicine compared the meridian systems side by side using anatomical analysis. In eight out of nine comparisons, the myofascial and acupuncture pathways covered substantially the same territory. The Spiral Line, notably, appears to combine two acupuncture meridians into a single myofascial pathway [5].
The Urinary Bladder sinew channel is the clearest example. Classically, it runs from the foot to the head along the posterior body, branching through the posterior leg, lateral hip, lumbar and thoracic spine, and the occiput. Myers' Superficial Back Line covers almost exactly the same territory: plantar fascia, gastrocnemius, hamstrings, sacrotuberous ligament, thoracolumbar fascia, erector spinae, suboccipitals, galea aponeurotica. When you put the anatomical diagrams side by side, you're looking at two different cartographers mapping the same coastline.
A 2016 systematic review by Wilke et al. provided the first solid scientific evidence for the existence of myofascial meridians, with the strongest support for the Superficial Back Line and the functional lines [4]. Myers himself has noted that the myofascial meridians and the oriental meridian lines are not equivalent — they overlap, but they don't perfectly coincide [7]. The sinew channels, as classically described, don't account for the full complexity of the fascial system, and the fascial system doesn't fully account for everything the sinew channels describe. They're parallel maps, not the same map.
Myofascial meridians:
Continuous lines of pull through the body's fascial network, as described in Thomas Myers' Anatomy Trains model. Each meridian links multiple muscles and connective tissue structures into a single tensional unit that transmits force across regions that would otherwise seem anatomically unrelated. The nine primary myofascial meridians include the Superficial Back Line, Superficial Front Line, Lateral Line, Spiral Line, Arm Lines, and the Deep Front Line. They are supported by anatomical dissection and, increasingly, by in-vivo imaging and mechanical testing, though the evidence base varies by line.
What the Fascia Research Adds
Acupuncture points and meridians correspond significantly to connective tissue planes, providing a structural rather than purely philosophical basis for the classical meridian maps. Dr. Helene Langevin, now Director of the National Center for Complementary and Integrative Health at the NIH, published a 2002 paper in The Anatomical Record finding exactly this correspondence [1]. Her research showed that acupuncture needles, when manipulated, cause connective tissue to wind around the needle — a mechanical signal that transmits into the tissue at distances of up to 4 centimetres from the insertion site [2].
Later research found that approximately 80% of acupuncture points in the arm are located at sites where fascial layers intersect [1]. These aren't random anatomical coordinates. They sit at places where mechanical input propagates furthest and fastest through the connective tissue network.
This is where the dots connect. If acupuncture points are concentrated at fascial junctions, and meridians follow fascial planes, and the fascial planes correspond closely to the sinew channels, and the sinew channels overlap substantially with myofascial lines — then what you have isn't Eastern mysticism facing off against Western science. You have two traditions, separated by 2,000 years and different epistemologies, describing the same architecture. The clinical reasoning behind fascial assessment and the clinical reasoning behind sinew channel work start to look like the same conversation in different languages.
For the fascial anatomy underpinning this work in more depth, A Field Guide to Fascia covers the tissue physiology, sensory layers, and clinical application. 1 CE credit, fully online.

Acupuncture points on the arm cluster at sites where fascial layers intersect, suggesting a structural basis for the meridian system.
What This Means in Practice
When local treatment of a symptomatic region fails to produce lasting results, tracing the sinew channel or myofascial line through which that region is loaded often reveals the upstream or downstream source of the pattern. Take a practitioner treating chronic low back pain — common enough that it barely needs an introduction. She's working with a client whose lumbar complaints keep returning despite solid local work. The paraspinals release. The SIJ mobilizes. Within a week the client is tight again.
Thinking purely segmentally, she keeps going back to the lumbar region. Thinking in fascial lines or sinew channels, she starts asking different questions. Where is the posterior line loaded? Is there plantar restriction feeding tension up the Superficial Back Line and Bladder sinew channel? Is the sacrotuberous ligament the missing link? Are the suboccipitals cranking on the top of the line and pulling everything taut from above?
This is the practical value of understanding the overlap. It doesn't require believing in qi as a metaphysical substance. It doesn't require abandoning your anatomy. It asks you to take seriously the clinical observation that bodies transmit force across distances, and that the people who mapped those transmission lines two millennia ago were observing real phenomena, even if they had different words for them.
As an acupuncturist, I've found that treating sinew channels with an understanding of myofascial continuity produces more durable results than treating either system in isolation. As an RMT, knowing that the classical Bladder channel and the Superficial Back Line are essentially the same structure gives you a broader map to work from when local treatment isn't holding.
The question isn't whether ancient practitioners understood fascia. They didn't, not in those terms. The question is whether they observed the body carefully enough, over enough time, to map something real. Based on where the research is landing, the answer appears to be yes.
A Field Guide to Fascia covers the full fascial anatomy underlying this work, including the sensory and proprioceptive layers that make both systems clinically coherent. 1 CE credit, fully online. The Acupressure and Meridian Massage course covers the full clinical protocol for working with the meridian system in manual therapy practice.
References
[1] Langevin, H.M., & Yandow, J.A. "Relationship of acupuncture points and meridians to connective tissue planes." The Anatomical Record, 269(6), 257–265. 2002.
[2] Langevin, H.M., Churchill, D.L., Wu, J., Badger, G.J., Yandow, J.A., Fox, J.R., & Krag, M.H. "Evidence of connective tissue involvement in acupuncture." The FASEB Journal, 16(8), 872–874. 2002. https://doi.org/10.1096/fj.01-0925fje
[3] Stecco, A., Macchi, V., Stecco, C., Porzionato, A., Ann Day, J., Delmas, V., & De Caro, R. "Anatomical study of myofascial continuity in the anterior region of the upper limb." Journal of Bodywork and Movement Therapies, 13(1), 53–62. 2009.
[4] Wilke, J., Krause, F., Vogt, L., & Banzer, W. "What is evidence-based about myofascial chains: A systematic review." Archives of Physical Medicine and Rehabilitation, 97(3), 454–461. 2016. https://doi.org/10.1016/j.apmr.2015.07.023
[5] Dorsher, P.T., & Fleckenstein, J. "Myofascial meridians as anatomical evidence of acupuncture channels." Journal of Alternative and Complementary Medicine, 15(9), 1019. 2009.
[6] Queiroz Lemos, B., Morais-Ribeiro, R., Fernandes de Oliveira, L., & Fuentes Désir, J. "Correlation between the sinew channels with the myofascial system, pathology, and treatment." Journal of Acupuncture and Meridian Studies, 15(4), 201–208. 2022.
[7] Myers, T.W. Anatomy Trains: Myofascial Meridians for Manual and Movement Therapists (3rd ed.). Churchill Livingstone. 2014.